
Limiting Loans, Limiting Access
The Future of the Rehab Workforce

The US Department of Education released its final rule related to changes to the federal student loan system after initial negotiations from the The Reimagining and Improving Student Education (RISE) Committee in the Fall of 2025.
The final rule can be found here. In the coming weeks and months, we will see many articles and posts written about this final rule. Many will be written by AI, and many will be written by people that didn’t read the language in the decision themselves. I encourage everyone in academia to read these documents in full. To read the language that was used, and to understand the changes for themselves.
These loan changes will affect almost everyone that pursues higher education (that doesn’t come from a family with enough wealth to pay for education out of pocket). It will also impact all of us that work in higher education. I believe it will also impact those in clinical care that rely on clinical education programs to support their clinic volume.
Here are the major points from the decision I believe are most crucial to understand:
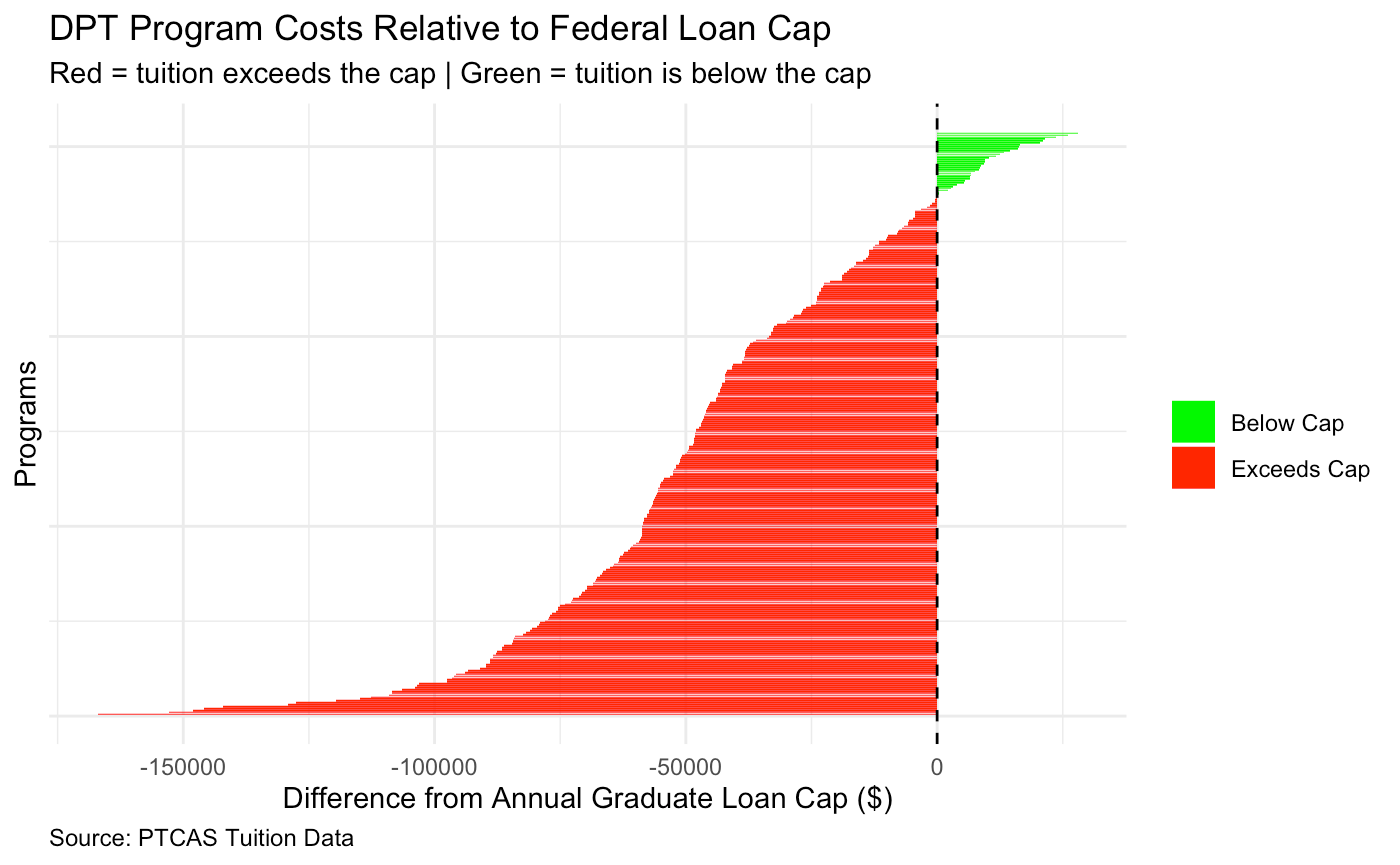
Graduate student loans are capped annually at $20,500, with an aggregate cap of $100,000
For the first time, Parent PLUS borrowers are capped annually at $20,000, with an aggregate cap of $65,000 per dependent
Rehabilitation degrees (PT, OT) will be considered graduate student loans rather than professional (which would up the cap to $200,000).
Now there are substantial changes to loan repayment options which will move into 2 (instead of the prior 16 or so) repayment options: Tiered Standard plan and the Repayment Assistance Plan (RAP). This is important, but the major upset with this news relates to the decision to consider only a narrow definition of a professional degree within the final rule.
I am going to dive into this part a bit more because the language (in my opinion) is more infuriating than the actual decision. The decision maintains that the original 11 core professional degrees will be counted (pharmacy (Pharm.D.), dentistry (D.D.S. or D.M.D.), veterinary medicine (D.V.M.), chiropractic (D.C. or D.C.M.), law (L.L.B. or J.D.), medicine (M.D.), optometry (O.D.), osteopathic medicine (D.O.), podiatry (D.P.M., D.P., or Pod.D.), theology (M.Div., or M.H.L.), and clinical psychology (Psy.D. or Ph.D.)), with the addition of a “multi-part test” to see if any other degrees count. This is the infuriating part.
The multi-part test has 4 components:
Signifies both completion of the academic requirements for beginning practice in a given profession, and a level of professional skill beyond that normally required for a bachelor's degree
Is generally at the doctoral level, 5 and that requires at least six academic years of postsecondary education coursework for completion, including at least two years of postbaccalaureate level coursework
Generally requires professional licensure to begin practice
Is within a four-digit Classification of Instructional Programs (CIP) code in the same intermediate group as the core list of 11 program fields.
A Doctor of Physical Therapy Degree (DPT) meets the first three specifications very clearly. The fourth specification is the one that requires some more investigation. A full list of CIP codes can be found here. “Within a four-digit CIP code” essentially means, the degree must start with the same four digits as one of the existing 11 professional programs. So, PharmD is 51.2001, so anything that begins with 51.20 and meets the other three specifications in the test above, would be considered professional. Physical Therapy and Occupational Therapy fall under Rehabilitation and Therapeutic Professions (51.23), and therefore, do not meet the criteria for a professional degree.
So, where does that leave us? It leaves us in a place where most of the DPT programs in the US are not going to be able to be afforded without students taking out private loans. To be more demonstrative of how many programs would actually be able to support students without any private loans, see this Figure which I created from PTCAS data. All programs in red would exceed the graduate cap.
However, this decision additionally has tremendous downstream implications for the diversity of our profession (which already has its many issues) as well as implications for availability. If fewer people can afford the degree, we will have fewer providers to care for our communities.
I am happy to see the APTA strongly opposing this decision. If you read this far, please take a minute to reach out to congress via this quick link:
I entered this profession with over $200,000 in student loans. I love this profession, and believe so much in what we can do for our patients and for our communities. I was able to pay off my loans in just 7 years because of the protections federal student loans provided. When I graduated, I felt so unsupported by those that entered before me. There was a strict divide between those that entered as a Bachelors or Masters and those that paid the higher rates for the DPT. Instead of feeling welcomed or mentored, I heard “well I wouldn’t have gone to school if I had to pay that much.” And now, we don’t just face a crisis for students, or a crisis of availability, but we face a new divide.
Those that entered before and after July 1, 2026.
But what good does it do to perpetuate that divide? I am seeing programs push up fall start dates just to get one more class in before this change. Don’t get me started on how useless that is in the long-run, but sure it’s nice for that one cohort of students you are trying to protect.
I believe the best thing we can do to protect our new graduates and incoming students is to agree we will continue to fight for them. This decision will not affect us—those that have been practicing and have paid off our loans years ago—in the same way it will affect our next generation. But it certainly will impact our profession and our patients. And for that, we must continue to oppose this. We must continue to think of creative ways to support our students and those that must borrow to enter this profession. And we must use language that doesn’t perpetuate this divide—especially as academics and mentors.